

By: Vaaragie Subramaniam, William Echols, Jessica Houck
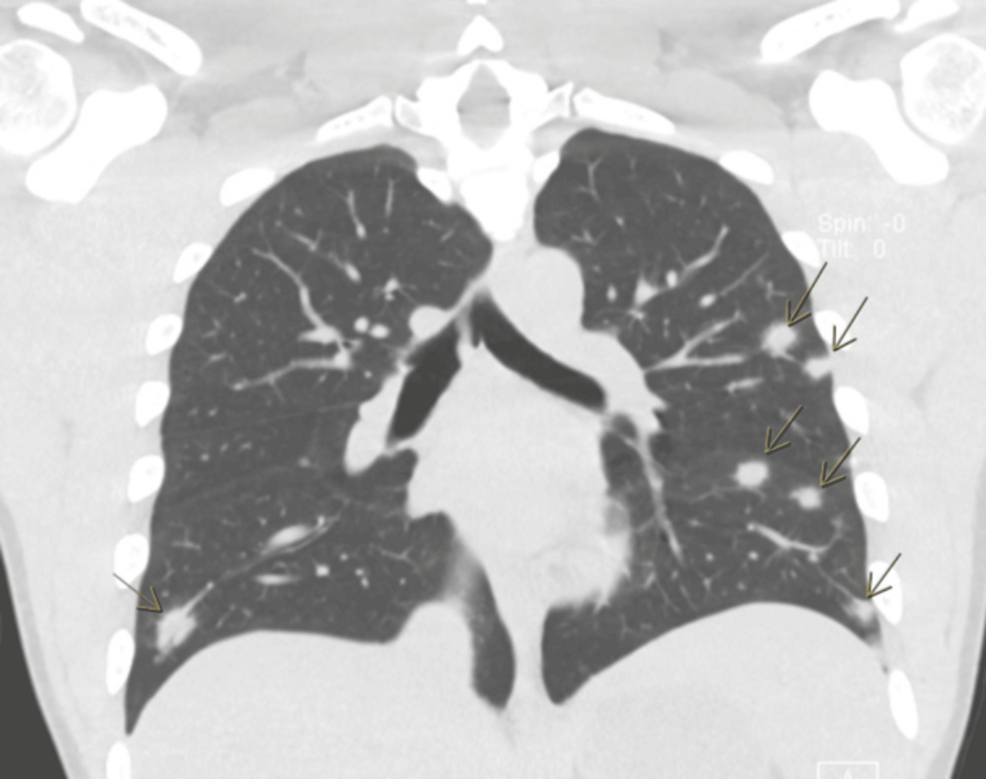
A 22-year-old African American male patient presented to the emergency department (ED) with blood-tinged vomiting and chest tightness. Workup in the ED showed acute renal failure with pulmonary septic emboli on computed tomography (CT) imaging. He was admitted to the hospital. During his hospital stay, aerobic/anaerobic venous blood cultures were positive for Fusobacterium necrophorum, and an ultrasound of the internal jugular vein revealed a deep vein thrombosis (DVT) consistent with septic thrombophlebitis. He was subsequently diagnosed with Lemierre syndrome. Evaluation for oropharyngeal disease, a more common cause, was negative, making this an atypical presentation. The patient was initially treated with piperacillin-tazobactam, then tailored to metronidazole based on susceptibility for four weeks, and had a full recovery.